
WHICH TREATMENT MEETS HOSPITAL REGULATORY REQUIREMENTS FOR PREVENTING OPPP’S?
J. Darrel Hicks
Owner at Safe, Clean and Disinfected
December 17, 2024
Water management programs in healthcare facilities are an important way to help protect vulnerable patient populations as well as staff and visitors. The Centers for Medicare & Medicaid Services, The Joint Commission, The Veterans Health Administration, and CDC consider it essential that hospitals and nursing homes have a water management program that is aligned with American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE) industry standards and limit Opportunistic Pathogens in Premise Plumbing (OPPP) from growing and spreading in their facility.
From plumbing to patients
Tap water meets stringent safety standards in the United States, but it is not sterile. Germs may be present when water leaves the tap. For typical household uses, these germs rarely pose a serious health risk.
However, in healthcare settings, water uses are more varied, and patients are more vulnerable to infection. Certain plumbing conditions can even encourage microbial growth, leading to dangerously high levels of potential pathogens. Healthcare facilities must evaluate their water use for its risk to harbor and transmit healthcare-associated pathogens.
MDROs in Drains
Recent evidence indicates sinks and other drains, such as toilets or hoppers, in healthcare facilities can become contaminated with multidrug-resistant organisms (MDROs). Because different types of bacteria may contaminate the same drain, drains can serve as sites where antimicrobial-resistant genes transfer between bacterial species.
Sink drains have been identified as important reservoirs for 16 multi-drug-resistant Gram-negative bacteria. Here, bacteria form biofilms in pipe lumens, from which cells may be released during sink use and spread outside the drains within droplets or as aerosols.
As a result, surfaces in the patient-care environment may become contaminated, which may lead to Healthcare Associated Infections (HAIs) and outbreaks. Bacterial drain reservoirs are difficult to eradicate, as commonly used hospital-grade disinfectants have no effect on these biofilms.
Disinfectants That Do not Kill Biofilm in Premise Plumbing
Biofilm- collections of microorganisms that stick to each other and adhere to surfaces in moist environments, like the insides of pipes. It can last in drains for long periods of time and are often difficult or even impossible to remove.
Pouring disinfectants into sinks has only a modest, transient effect because the disinfectants flow rapidly down the drain, providing inadequate contact time and poor penetration into areas harboring biofilm-associated bacteria, non-tuberculosis mycobacteria, non-fecal coliforms, fungi and protozoa.
There are >10,000 EPA-registered disinfectants. Of all these products there are only four chemistries—hypochlorous acid, bleach, peracetic acid and sodium di-chloro-iso-cyanurate—are effective against endospore forming bacteria such as C. diff.
A handful of large manufacturers produce these 4 basic chemistries, which then are private labeled by scores of companies. Search EPA Registration # to view the master label.
Sodium Dichloroisocyanurate (NaDCC) is a phenomenon because it has the unique ability to be more powerful at destroying biofilm, bacteria, viruses, and fungi like C. auris yet is safer than those mentioned previously. I am aware of NaDCC products that have both biofilm and C. auris claims while having a 0/0/0 hazard rating, neutral pH, and the lowest EPA toxicity category IV.
Foaming Disinfectants Are Superior to Liquid Disinfectants
Testing of a foam application of a 3.13% hydrogen peroxide and 0.05% peracetic acid disinfectant suppressed sink drain colonization significantly longer than poured liquid disinfectants, due to enhanced contact time and penetration into biofilm. The foam product is EPA-registered to kill Pseudomonas aeruginosa and Staphylococcus aureus biofilms with a 5-minute contact time. However, the optimal frequency of application is uncertain. Researchers proposed that a frequency of drain disinfection occur every 3-5 days to be effective.
Long-term effects on plumbing pipes were undetermined but would need to be studied further. A reduction to two log10 CFU was deemed effective. However, the level of reduction required to minimize the risk of dispersal (splashing) of organisms is uncertain. The cost of just the disinfectant for one treatment was estimated to be <$2.00 (not including labor). This is labor intensive and dependent on the manpower to apply the foam disinfectant regularly.
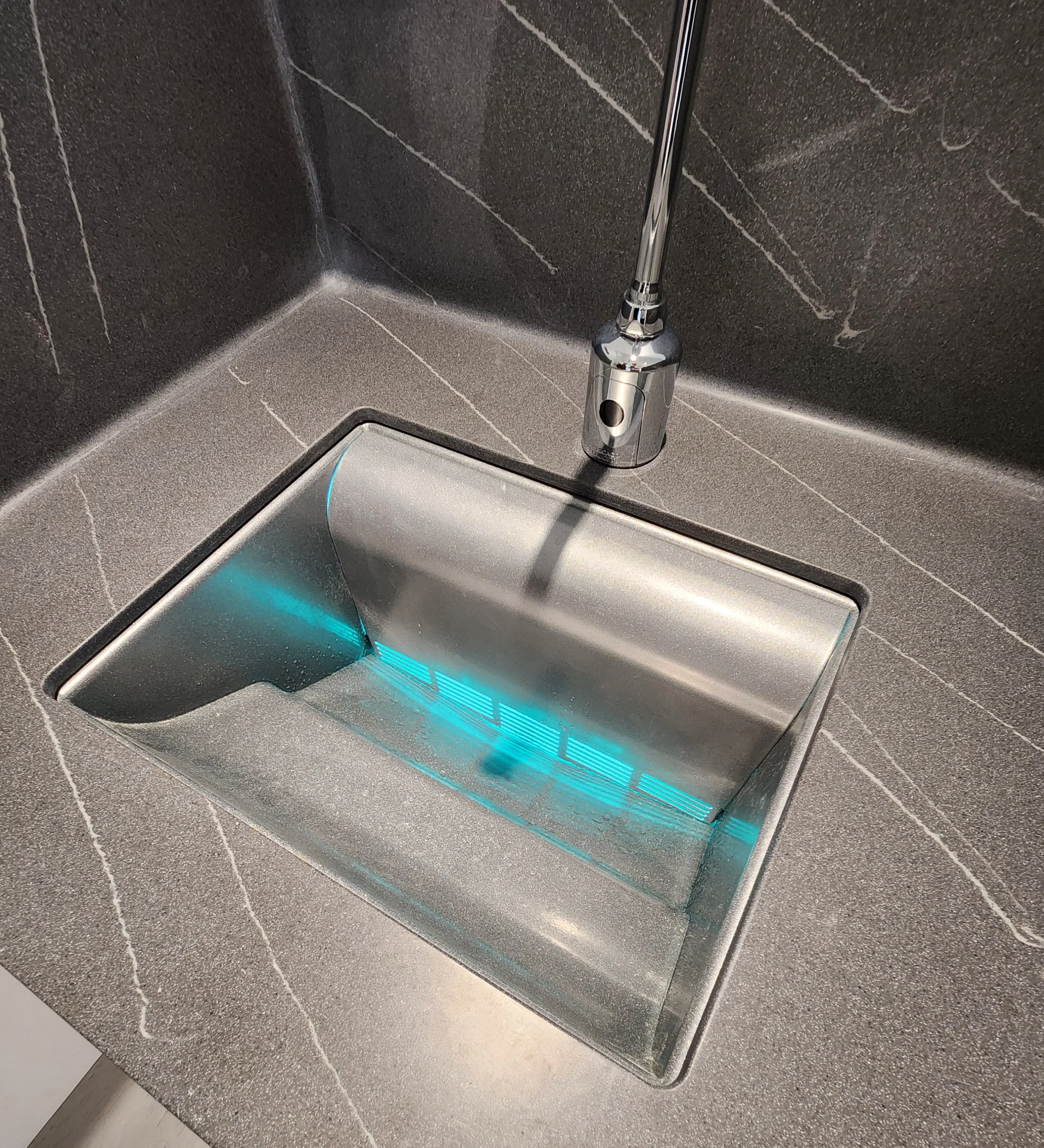
The BEST-IN-CLASS CAD Biofilm Eliminator is the ReSet265 Sink
When it comes to preventing biofilm from the p-trap to the sink drain, the ReSet265 sink is the only Continuously Active Disinfection (CAD) available on the market. As such, it is far superior to foaming disinfectants and it is here now (not in the future). In my professional opinion, the ReSet265 sink is the only “set it and forget it” infection prevention solution for wastewater management in hospital sinks.
CURVED SURFACE
For the first time this sink has implemented a curved surface to reduce splash by coordinating and matching the exact location of the surface with the discharge location of the faucet.
EXHAUST-NEGATIVE PRESSURE
First sink to ever incorporate exhaust through the basin into a negative pressure air chamber (ante room) above the sink trap.
GERMICIDAL ULTRA-VIOLET LIGHT
First sink to implement germicidal ultra-violet lights have been introduced within the negatively pressurized chamber (ante room) to kill bacteria located within the drain trap and within the ante room before they have a chance to contaminate the sink basin used by patients or hospital staff.
SANITIZING AGENT
First time a sink using one or more sanitizing agent injectors at various locations throughout the open cavity and/or into the exhaust port to help clean the surfaces of the open cavity and the exhaust port.
SMART CONTROLS
A central control system has been implemented to provide monitoring and control to ensure that the features of the sink are functioning according to their intended design.
SO, WHAT’S NEXT?
1. Contact Us-we would love to answer any questions you have and provide custom pricing for your specific needs.
2. Schedule an Installation-After placing an order, our sinks are ready to be installed by a plumbing company of your choice.
3. Start Saving Lives-7% does not seem like a big number. But when it happens in the ICU and adds an additional 26 days to their length of stay: that is HUGE. Twenty-four (40%) patients with Pseudomonas Aeruginosa-HAI died within 30 days of infection; PA-HAI was deemed to have caused death in two (3.3%) and contributed to death in and an additional 20 (33%).
In an ICU the daily cost of being treated for an HAI is $10,000. Adding 26 days to his/her length of stay would be $260,000 for one patient. A single hospital had 72 PA-HAI patients x $260,000 = $18,720,000. That is enough money to buy and install 3,120 ReSet265 sinks.
"In conclusion, based on this study, >7% of PA-HAI in ICUs may be attributable to sink drains, though sampling limitations may have led to underestimation of risk. With increasing antimicrobial resistance, attention to sink drains may still be an under-recognized source of bacteria causing HAIs."
For more information on the pricing of our sinks and a custom solution for your hospital, complete the form and somebody will quickly respond.
Or call Tom Hicks (402) 981-6365
Address this problem starting today and for the future!